The COVID-19 pandemic resulted in millions of deaths worldwide, affecting individuals of every age, ethnicity, gender, and economic status. This observation alone highlights the importance of examining this issue, as this outbreak has undeniably made a transformative impact within the sphere of public health. However, recent studies have determined that individuals of the male sex have died from COVID-19 complications at a noticeably higher rate than their female counterparts (Klein et al., 2020). Klein et al. (2020) found that this phenomenon has occurred due to a combination of biological, behavioral, and social factors, thus demonstrating the importance of analyzing quantitative and qualitative data to reduce inequities in future public health emergencies.
Moosazadeh et al. (2025) found that sex differences in COVID-19 mortality are driven by distinct molecular mechanisms. Males show downregulation of genes involved in hydrolase activity, which weakens lung immune and antimicrobial responses. Females, on the other hand, have enriched hydrolase-related genes, contributing to stronger immunity and better outcomes. Males also exhibit upregulation of AGTR1 and ADAM-17, which influence ACE2 activity and SARS-CoV-2 shedding, potentially facilitating viral entry and worsening lung injury (Moosazadeh et al., 2025). Furthermore, SARS-CoV-2 uses ACE2 and TMPRSS2 to enter host cells. ACE2 is more highly expressed in male lungs, and TMPRSS2 is regulated by androgens, increasing male susceptibility. In contrast, estrogen may protect females by modulating immune responses, while testosterone can exacerbate inflammation in males (Moosazadeh et al., 2025).
Kharroubi and Diab-El-Harake (2024) determined that males are more likely to engage in high-risk activities that increase their chances of dying from COVID-19, including tobacco use and alcohol consumption. Auderset et al. (2024) also found that unhealthy diets and societal norms discouraging timely medical care predispose men to obesity, diabetes, and similar health issues, which heighten the risk of severe COVID-19. Lastly, men are less likely than women to avoid large gatherings and seek medical care (Kharroubi & Diab-El-Harake, 2024). Men also work in hazardous industries at a higher rate than women, which increases their chances of facing severe COVID-19 complications (Auderset et al., 2024).
These research findings reveal that men are more likely to die from COVID-19 due to a myriad of factors. However, it remains unclear which demographic subgroups of men are most at risk of dying from COVID-19. I intend to discover this information by answering three questions.
1. How do COVID-19 mortality rates differ between men and women across age groups?
Age is a key predictor of COVID-19 severity and death. Breaking down data by sex and age can reveal whether higher male mortality occurs across all ages or mainly among older men, which is vital for targeted interventions, resource allocation, and risk communication.
2. Which U.S. states report the highest male COVID-19 mortality counts?
This question is important to answer because identifying states with the highest male COVID-19 mortality counts can reveal regional disparities in health outcomes. Understanding these patterns helps target public health interventions, allocate resources effectively, and develop policies tailored to high-risk populations. Additionally, it can shed light on underlying social, economic, and environmental factors contributing to increased male mortality across different states.
3. How do male COVID-19 mortality rates vary across race and ethnicities?
Understanding how male COVID-19 mortality rates vary across race and ethnicity is important because it reveals deep health inequities that go beyond biological differences. Racial and ethnic minority men experienced disproportionately higher mortality rates during the pandemic, often due to structural factors such as unequal access to healthcare, higher likelihood of working in high-risk or essential jobs, crowded living conditions, and a greater burden of underlying health conditions. Examining these differences helps highlight the role of social determinants of health and prevents broad conclusions about men as a single risk group.
The Provisional COVID-19 Deaths by Sex and Age dataset contains counts of deaths involving COVID-19 in the United States, disaggregated by sex and age group. The data are derived from death certificate information reported to the CDC’s National Center for Health Statistics (NCHS) and include cases in which COVID-19 is listed as an underlying or contributing cause of death. This dataset enables analysis of mortality patterns across different age groups and between males and females, supporting demographic comparisons of COVID-19 mortality burden at the national level.
The COVID-19 Weekly Cases and Deaths by Age, Race/Ethnicity, and Sex dataset provides weekly counts of COVID-19 cases and deaths in the United States, stratified by age group, race/ethnicity, and sex. This dataset allows for intersectional analysis of how COVID-19 outcomes varied across demographic groups and over time. By including both cases and deaths, it supports comparisons between infection trends and mortality outcomes, offering insight into disparities in disease impact across populations.
Data preparation began with importing the datasets into Tableau and conducting an initial assessment of variable definitions and data completeness. Records with missing or unspecified demographic information were filtered to minimize bias and improve interpretability. Relevant variables related to sex, age, race, ethnicity, and time were selected to align with the study’s analytical objectives. The data were then structured to enable consistent comparisons of COVID-19 mortality patterns across demographic groups, supporting reliable visualization and analysis of disparities in male COVID-19 outcomes.

Figure 1. COVID-19 Deaths of Men and Women Across Age Groups
Across all age groups, COVID-19 claimed more lives among men (3,787,934) than women (3,109,748). In other words, roughly 54.9% of deaths were male, whereas 45.1% were female. The male-to-female death ratio was approximately 1.22:1, indicating that for every death among women, approximately 1.22 men died from COVID-19. Interestingly enough, more women over the age of 85 (1,045,997) died from COVID-19 than men in the same age group (825,540), representing approximately 26.7% more deaths among women.
However, men experience more deaths in the remaining age groups. For instance, men aged 75-84 faced 1,008,553 deaths, whereas women in the same age group experienced 792,288 deaths. This represents a striking 27.3% higher death rate among men. In the 65-74 age group, male COVID-19 deaths were 1.45 times higher than female deaths. A similar pattern is seen in the other age groups, reflected by the wider layers in the male bars.
Based on this visualization, older men are more likely to die from COVID-19 than their younger counterparts. The likelihood of COVID-19 death among males largely increases between the 45-54 and 55-64 age groups, rising by approximately 179%. This indicates that this age range represents a critical point for increased risk.


Figures 2 and 3. Concentration of Male COVID-19 Deaths in the United States
Both the bar chart and map show that California, Texas, and Florida have the highest COVID-19 mortality count for men. On the other hand, Vermont and Alaska have the lowest male COVID-19 mortality count. It is likely that these differences are driven by variations in population size and density, as well as differences in occupational exposure and public health responses across states.
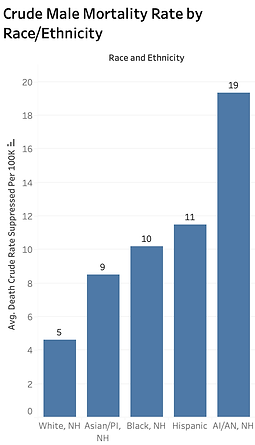
Figure 4. Crude Male Mortality Rate by Race/Ethnicity
The visualization shows clear disparities in average crude male mortality rates per 100,000 across racial and ethnic groups. American Indian/Alaskan Native males have the highest mortality rate, which is nearly four times higher than that of white males.
Altogether, the visualizations highlight profound and persistent health inequities during the COVID-19 pandemic, demonstrating that mortality was not evenly distributed across the U.S. population. Analyzing the data across gender, age, geography, and race reveals how biological factors, regional differences, and systemic inequalities combined to create uneven COVID-19 mortality risks. Across nearly all adult age groups, males experienced significantly higher COVID-19 mortality rates than females. Although mortality rose sharply with age for both sexes, men consistently experienced higher death rates, with the greatest gender gap occurring in middle-aged adults. This pattern indicates that being male acted as an independent risk factor in addition to age.
Geographic patterns further reveal sharp state-level differences in male COVID-19 mortality. Highly populated states such as California, Texas, and Florida reported the greatest number of deaths. High male mortality in states like California, Texas, and Florida reflects their large populations, high urban density, and greater opportunities for virus transmission. Differences in healthcare capacity, public health measures, and timing of outbreaks also contributed to these geographic variations.
Racial and ethnic disparities were the most striking, particularly among American Indian and Alaskan Native males. Elevated mortality rates among Hispanic and Indigenous populations persisted even after age adjustment, reflecting deep-rooted structural inequities such as limited healthcare access, higher frontline employment, and housing conditions that increased exposure risk.
In conclusion, these visualizations show that COVID-19 mortality in the U.S. was shaped by both biology and systemic disparities. Higher death rates among men, the elderly, and American Indian/Alaska Native populations highlight how social and structural factors influenced outcomes. This analysis emphasizes the need for targeted interventions and equitable resource distribution to protect vulnerable communities in future public health crises.
Auderset, D., Amiguet, M., Clair, C., Riou, J., Pittet, V., Schwarz, J., & Mueller, Y. (2024, May 20). Gender/sex disparities in the COVID-19 cascade from testing to mortality: An intersectional analysis of Swiss surveillance data. SSPH+. https://www.ssph-journal.org/journals/international-journal-of-public-health/articles/10.3389/ijph.2024.1607063/full
Kharroubi, S. A., & Diab-El-Harake, M. (2024, July 9). Sex differences in COVID-19 mortality: A large US-based cohort study (2020–2022). AIMS Public Health, 11(3), 886–904. https://doi.org/10.3934/publichealth.2024045
Klein, S. L., Dhakal, S., Ursin, R. L., Deshpande, S., Sandberg, K., & Mauvais-Jarvis, F. (2020, June 22). Biological sex impacts COVID-19 outcomes. PLOS Pathogens, 16(6), e1008570. https://doi.org/10.1371/journal.ppat.1008570
Moosazadeh, M., Ghadirzadeh, E., Saeedi, M., Mousavi, S. A., Rouhanizadeh, H., Alizadeh-Navaei, R., Yazdani Charati, J., Tirgar Fakheri, H., Hedayatizadeh-Omran, A., Majidi, H., Alikhani, A., Rafiei, A., Aliyali, M., Erfani, Z., Gheibi, M., Parsaee, M. R., Khademloo, M., Mousavi, S. J., Yousefi, S. S., … Assadi, T. (2025, October 28). Sex-based differences in mortality among a large cohort of hospitalized patients with RT-PCR-confirmed SARS-CoV-2 infection at five different pandemic waves in northern Iran. Scientific Reports, 15, Article 21553. https://www.nature.com/articles/s41598-025-21553-x